This is an online e log of patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.This elog also reflects my patient centered online learning portfolio








I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan
80 yr old male, unemployed from nampel came to opd with
C/o-
nocturia(5times/day)
Burning micturition
Pain in abdomen during micturtion
Dysuria since 1 day
History of presenting illness
Patient was apparently asymptomatic before July 2021
Then he developed nocturia(5times /day), urgency, urgency incontinence, dribbling, poor stream for 2 months (June-sep of 2021). Patient went on acute retention of urine in sep 2021 and was catherized.
He gives a history of voiding trial given 5 months back and failed and he was advised for surgery but he refused it.
Hematuria was seen when he collected urine for urine examination.
Dysuria since 1 day, 2 episodes of vomiting 2 days back.
Glucose levels raised to 540 yesterday night
No history of fever, loss of appetite, loss of weight, turbiduria
Past history
He is known case of diabetes mellitus
2 yrs back he was diagnosed to have HTN but he refuged to take medications
Not a k/c/o , Asthma, TB, thyroid
Treatment history :
He is on medication for diabetis since 2 and 1/2 yrs
Personal history:
Married, unemployed, normal appetite, mixed diet, normal bowel, burning micturition, no known allergies
Alcoholic but stopped consumption since 2 yrs.
No significant family history
Examination :
General Examination :
Patient is conscious, coherent and coperative well built and well nourished.
No pallor, icterus, cyanosis, clubbing of fingers, lymphadenopathy, pedal edema
Systemic examination:
PER ABDOMINAL EXAMINATION:
INSPECTION-
Shape of abdomen : flat
Umbilicus : inverted
All quadrants of abdomen move with respiration
No visible peristalsis, pulsations, sinuses, engorged veins, hernial sites c, no scar on the abdomen
PALPATION-
Abdomen soft
No local rise of temperature
No tenderness
No organomegaly
PERCUSSION:
Resonant note heard over all quadrants.
AUSCULTATION:
Bowel sounds heard
CVS EXAMINATION:
INSPECTION
The chest wall is bilaterally symmetrical
No dilated veins, scars or sinuses are seen
Apical impulse not visible
PALPATION:
Apex beat localised
AUSCULTATION:
S1 and S2 heard
No Murmurs
RS EXAMINATION:
INSPECTION:
Shape of chest: bilaterally symmetrical
Expansion of chest: Equal on both sides
Position of trachea: Central
No visible scars, sinuses, pulsations
PALPATION:
Inspectory findings confirmed
No tenderness, local rise of temperature
Normal expansion of chest on both sides in all areas
Position of trachea: Central
Vocal fremitus: resonant note felt
PERCUSSION:
Resonant note heard over all areas
AUSCULTATION:
Slight wheezing sound is heard
Vocal resonance: resonant in all areas
CNS EXAMINATION:
HIGHER MENTAL FUNCTIONS-
Normal
Memory intact
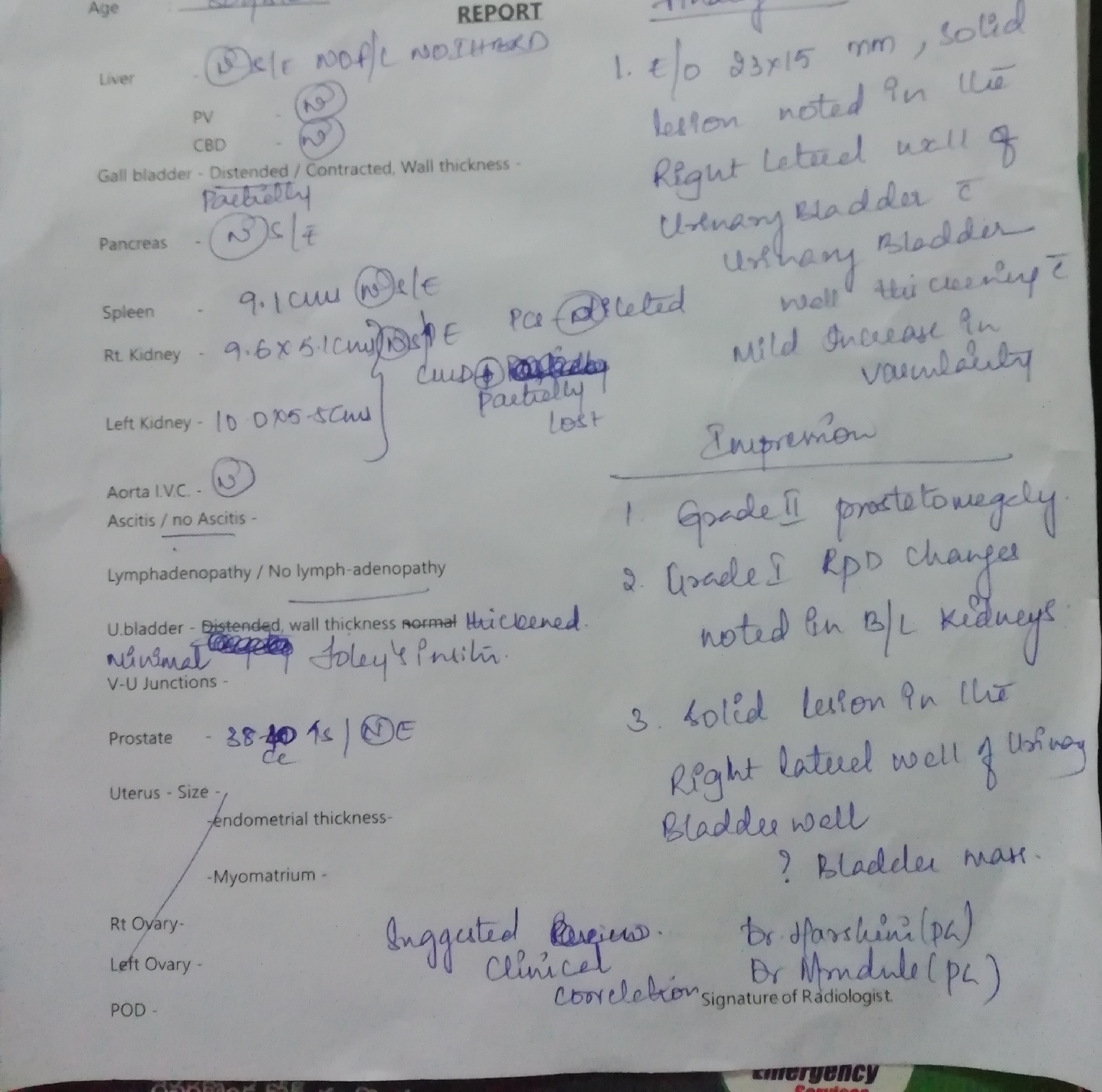
Investigations

Comments
Post a Comment