GENERAL MEDICINE (50F c/o generalised weakness )
This is an online e log book to discuss our patient d.e-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global onlin'e community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
A 50 year old female farmer by occupation presented to the OPD with
CHIEF COMPLAINTS:
-generalised weakness since 1 year
- loss of appetite since 1 year
- hematuria since 2 days
- dizziness since 6 months
- sob ( grade 2) since 6 months
- fever since 1 week
- itching on right side of neck since 1 month
HISTORY OF PRESENTING ILLNESS :
Patient was apparently asymptomatic 2 years back where she developed swelling of left lower limb first as with pain and then swelling progressed to whole body where she got admitted to Osmania and treated and swelling subsided and patient is doing fine after 1 year of that event patient gradually developed generalised weakness, easy fatiguability, loss of appetite,weight loss, sob ( grade 2-3) not with cough, cold , palpitations,
She developed itching on right side of neck since one month which is painless.
She has fever which is intermittent, low grade not associated with chills and rigors
She also has Hematuria for which she went to local hospital where she found to have Anemia for which she was transfused 5 units of blood in a span of 20 days and was discharged.
She was doing fine.
Since 6 months patient is experiencing similar complaints and went to hospital where she was found to have Anemia and got transfused 2 units of blood and came here as they were unsatisfied with the treatment there . She was admitted on Saturday July 08
PAST HISTORY:
Not a known case of HTN, DM 2 , CVA, CAD, TB , EPILEPSY ETC
She underwent hysterectomy surgery at the age 36 years after the third childbirth
PERSONAL HISTORY:
mother of 3 children ( 2 sons and 1 daughter)
Diet - mixed
Appetite- decreased since 1 year
Bowel and bladder- regular
Sleep-adequate
Allergies - No
MENSTRUAL HISTORY:
Menarche - 13 years age
Past - A Regular cycle 5/30
Present - hysterectomy done at the age of 36 yrs
Daily routine :
She wakes up at 5 o clock and does her daily activities and then she prepares for breakfast and have her breakfast at 7 o clock and then goes f.or work and at 12 o clock she haves her lunch near the field and in the evening she goes to home at 7 o clock and prepares for dinner and eats dinner and then goes to bed at 9-10 pm
After symptoms:
She is not going to any work since 1 and half year she stays at home and takes rest .
GENERAL EXAMINATION:
Patient is concious , coherent and cooperative well oriented to time place and person
Poorly built and poorly nourished
Patient was examined in a well lit room and after taking consent with adequate exposure .





Pallor -present
Icterus - positive
Cyanosis - negative
Kolinychia - negative
Clubbing - negative
Generalised lympadenopathy - negative
Edema - negative
VITALS:
BP- 90/60mmhg
PR- 84bpm
RR- 16 cpm
Rs- BAE +ve , NVBS
CVS- S1 S2 heard , no murmurs
CNS - NFND
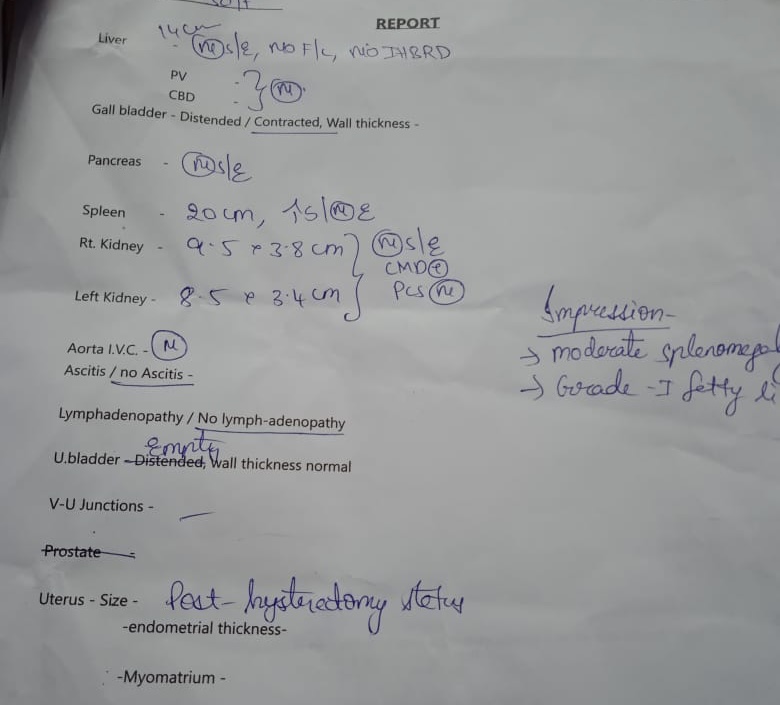
P/A - spleenomegaly
Size- 17.5 * 15 cms
Surface - smooth
Consistency - firm
Borders- rounded borders



Spo2 - 98% at RA
Temp- afebrile
CNS: NFND
CVS-S1,S2 heard ,no murmurs
RS- BAE present, NVBS Heard, no added sounds
P/A- spleenomegaly
PROVISIONAL DIAGNOSIS:
PANCYTOPENIA UNDER EVALUATION
? AKI ( pre renal)
Denovo HBSAG positive
Auto immune haemolytic anaemia ?
INVESTIGATIONS-















TREATMENT :
Tab.dolo 650mg po/sos
Sup.aristozyme 10ml po/tid
Tab.orofer XT po/OD
Temp monitoring 4th hrly
Vitals monitoring 4th hrly

S: Stools passed
No fever spikes
Tingling and numbness present
O:
Pt is conscious,coherent and cooperative
No pallor,icterus,cyanosis,clubbing,
lymphadenopathy,edema
Bp-100/60mmHg
Pr-84bpm
Temperature - Afebrile
Rr-16 cpm
CNS: NFND
CVS-S1,S2 heard ,no murmurs
RS- BAE present, NVBS Heard, no added sounds
P/A- spleenomegaly
A:
Pancytopenia under evaluation. ?AKI ( Pre-renal)
DENOVO HBsAg +ve
P:
- T.Dolo 650mg PO/SOS
- Syp. ARISTOZYME 10ml PO/TID
-inj.vitcofol 1ml IM/OD
- Temperature monitoring 4th hourly
- Vitals monitoring 4th hourly


Comments
Post a Comment